
Frailty Pathway
What is the Frailty Referral Pathway?
The clinical pathway for Frailty is designed to deliver holistic, person-centered care across the continuum of healthcare services, spanning hospital, community, and primary care settings. This pathway emphasizes early identification, proactive intervention, and multidisciplinary collaboration to address the complex needs of individuals living with frailty.
Current State
Community-dwelling older adults living with multiple co-morbidities and/or impacted by social determinants of health are among KLH-OHT priority populations.
Older adults constitute 28% of the total population in Kawartha Lakes, and 32% of the total population in Haliburton County, both significantly higher than the Provincial average of approximately 18%. Many of these individuals are living with multiple, chronic and complex health & social conditions including frailty and dementia.

Care Pathways Decision Tree
Select the most appropriate decision tree based on where the patient resides. If you have any questions about the Frailty Pathway or would like help setting up the referral destinations in Ocean, reach out to info@klhpcn.ca
Download (Microsoft Word):
What is Frailty?
According to the Canadian Frailty Network, frailty is a state of increased vulnerability, with reduced physical reserve and loss of function across multiple body systems. Frailty is a predictor of death, heightened vulnerability, institutionalization and a reduced quality of life.
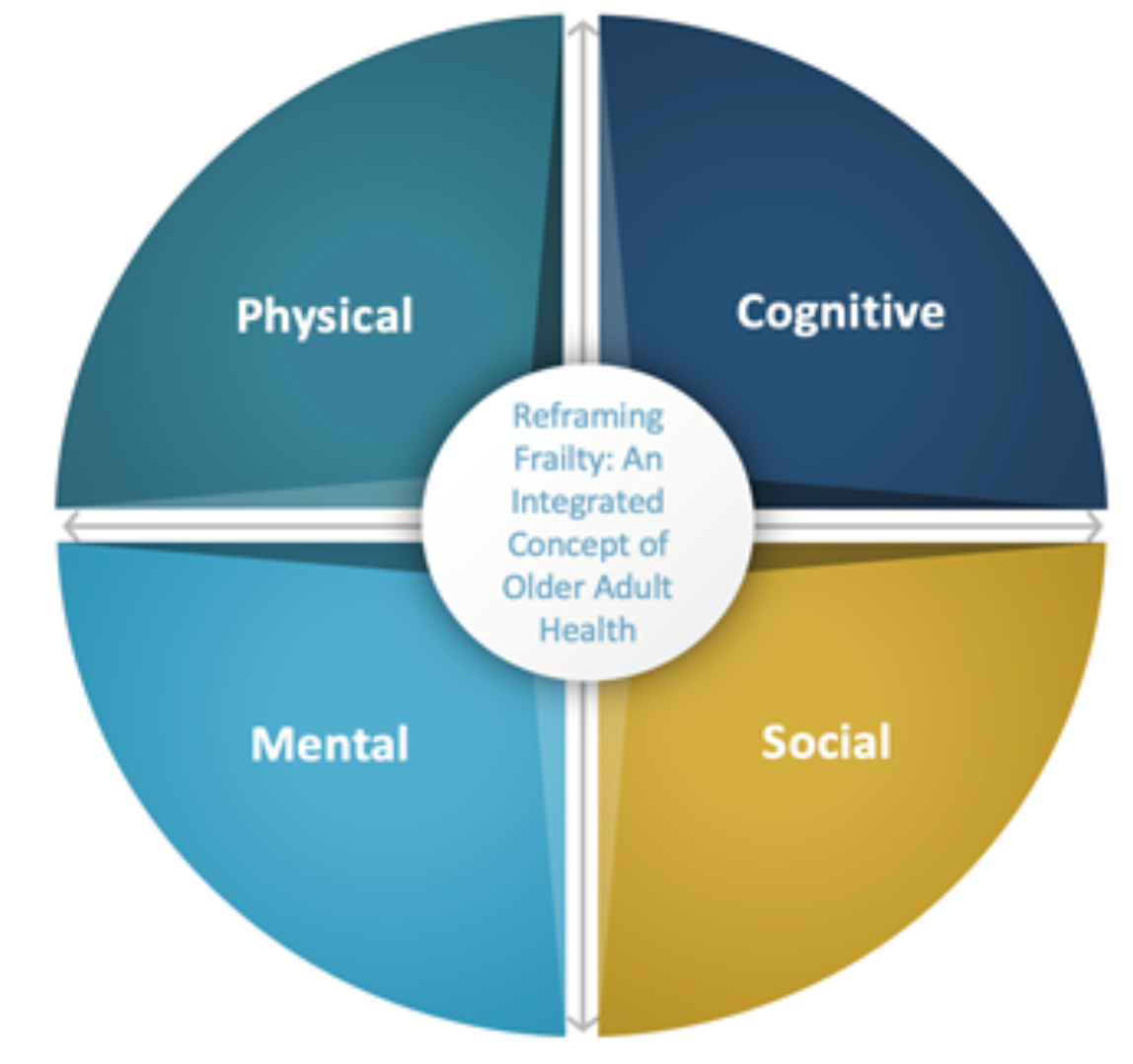
As proposed by the Ontario Collaborative of Aging Well, the concept of frailty must include the physical, cognitive, mental, and social health of older adults and their care partners, and the interaction and integration of these four domains.

Unmanaged frailty is among the drivers of Alternate Level of Care (ALC) rates in the province. According to the Provincial Geriatrics Leadership Ontario, by 2030, individuals living with frailty are estimated to rise by at least 20%; this is important as we recognize that even in the current state, we at KLH-OHT, do not have the ideal pool of community resources to best meet the needs of this clientele.
Source: PGLO 2023
An innovative solution.
Evidence suggests that implementation of proactive frailty screening & identification, and promotion of self-management strategies to prevent or stabilize frailty, directly contribute towards reducing unexpected hospitalizations, ALC designation, and the expression of LTC need.
Frailty screening can be leveraged to facilitate timely and coordinated access to a suite of preventative and specialized programs; as an upstream ALC avoidance strategy. All system partners including primary care can play a pivotal role in frailty management.
Developed by Seniors Care Network, the Primary Care Frailty Pathways outline standardized approaches to prevention, identification, assessment, and management to support older adults with living in the community, and/or maintaining their function and independence.

Source: Seniors Care Network 2023
Total
28.5 hours over a minimum of 6 weeks
Need help?
Please reach out to info@klhpcn.ca for more information about how various digital solutions (such as e-forms, e-referrals, etc.) can be leveraged to implement these pathways within your existing clinical workflows.

